The Opioid Epidemic: From Freud to Fentanyl with Anna Lembke
[ad_1]source
[ad_2]
Methadone Clinic Nearby – Methadone Clinic New York City – Methadone Clinics USA
Methadone Clinic Nearby – Methadone Clinic New York City – Methadone Clinics USA
Join us on Thursday, September 22 at 3:30pm CT for a live discussion with Dr. W. Michael Hooten, an aesthesiologist and pain management expert at Mayo …
source
Methadone Clinic In My Area – Methadone Clinics New York – Methadone Clinics USA
[ad_1]


Alcoholism and addiction in general are neither a defect of the character nor a weakness of self-control. It is a disease. And, if you’re like most of us, you’ve probably been affected. Maybe you are struggling with alcohol yourself or have a friend or family member who does. I rarely talk to someone who has no personal history of how addiction has affected their lives.
In fact, about 14 million adults have an alcohol-related disorder and there are about 95,000 alcohol-related deaths each year in that country.
Unfortunately, we don’t think of it like any other medical condition, so we don’t usually talk about it with our primary care physician. But this is one of the best places to start the conversation, during the annual review, when you talk about health goals. not bad to say, “I think I have a problem with alcohol.”
Some of the warning signs to look for in yourself or a loved one include sacrificing family ties for your addiction, such as missing a child’s ball game, concert, or graduation. The things you used to be passionate about fall by the wayside. You are tired and foggy, you can barely get up in the morning. You feel like the substance. Count down the time until you can get out of work and have a drink. You are in danger of losing your job or important relationships or you have had problems with the law. You tell yourself and others that you could easily quit smoking; but you never do.
By starting the conversation, you will have a clearer path to the help you need. Your doctor can guide you to outpatient support or counseling groups, or perhaps treatment at a center.
There is an overlap between behavioral health and addiction in terms of risk factors. Like behavioral health, addiction has a genetic heritability of approximately 60%. Mental health conditions and a history of trauma pose a higher risk of addiction. And the more health conditions you have, the sooner you start, the worse the disease will be. Those who start drinking before the age of 15 are five times more likely to develop an alcohol-related disorder.
I have spent my career talking and dealing with addiction. I see that the conversation is changing and it encourages me. There is a growing social awareness about addiction. We are more and more willing to have sincere and productive conversations about it.
The next time your doctor asks you about alcohol consumption, take it as an indication to have an honest conversation.
Matthew Stanley, DO, a psychiatrist from Sioux Falls, is a columnist and guest contributor to Prairie Doc this week on the Prairie Doc TV show. To access the entire Prairie Doc library for free and easy, visit www.prairiedoc.org and follow Prairie Doc on Facebook with On Call with the Prairie Doc, a medical question-and-answer program that airs on Facebook and is ‘broadcasts on SDPB most Thursdays at 7pm central.
[ad_2]Methadone Clinic Nearby – Methadone Clinic New York City – Methadone Clinics USA
Methadone Clinics In My Area – Methadone Clinic New York – Methadone Clinics USA
For over 30 years, Joy battled addiction. Now with four years in recovery, she tells her story. To learn more about substance abuse treatment at Johns Hopkins …
source
Methadone Clinics Nearby – Methadone Clinics NYC – Methadone Clinics USA
[ad_1]
To study the exclusive effect of khat chewing and khat addiction rehabilitation therapy, ECG data were collected from healthy chewing subjects, control subjects, and khat-addicted subjects admitted to a rehabilitation center. Variations in ECG signal characteristics were extracted using signal processing techniques to analyze changes in cardiac activity. Figure 1 shows the general procedure used in this study.
figure 1
General study procedures.
For the effect of khat on heart activity study, a quasi-interventional design approach was used. Subjects were selected based on a pilot survey conducted to identify suitable subjects. Selection criteria and control procedures included (1) being able to comply with the restrictions and conditions of the study, such as not chewing khat and drinking alcohol for at least two days before the study, no coffee in the last 18 hours, no drink soda within the past 12 hours, and no tea within the past 8 hours, (2) being a young adult between the ages of 18 and 35 (people in this age group are frequent chewers and also relatively healthy at Ethiopia), (3) should not have a confirmed case of cardiovascular disease and is not taking any medication such as lopinavir, ritonavir, azithromycin that may affect cardiac activity (a diagnosis was made before the study) and (4 ) free from any other drug use such as cocaine, marijuana, cannabis and cigarettes. A total of 50 subjects (25 experimental and 25 control) were selected for this study. Among these, 38 of them were men, with 19 control subjects and 19 chewers; the remaining 12 were women, with 6 control subjects and 6 chewers. Its occupation includes students, health workers and civil servants.
Chewing and control subjects were matched using criteria such as sex, age, body mass index (BMI) and occupation. To achieve the perfect match, control subjects were selected based on chewers’ sex, age (±5 years), BMI (less than 18.5 as underweight, 18.5-24.9 as normal, 25 -29.9 as overweight and more than 30 as obesity). To reduce environmental factors that may alter cardiac activity, ECG signals from matched chewing and control participants were recorded sequentially. Before the ECG recording, all subjects were asked to have lunch. Each subject was instructed to take a 5-minute break to reduce the impact of any potential physical movement.
For the post-chewing session, khat leaves were initially prepared by removing any non-chewing components. Each chewer was given 100g of the same type of khat called “Kellechaa” which is the most available, preferred and consumed khat in Jimma city. Tea, coffee, soft drinks and smoking were prohibited during the chewing session. Both the intervention and control groups were exposed to similar intervention/care conditions. Post-chewing ECG data acquisition was carried out after 2 hours of chewing session. Peak arousal usually occurs 2 hours after the initial chewing session19. Chewers were also able to identify their period of highest arousal.
ECG data acquisition was then performed using Lead II while participants were in a conventional sitting ECG recording position. Appropriate techniques and strategies were applied to improve signal quality, electrode-skin interface conductivity, and reduce artifacts. Standard recording methods were used to set up the device and subjects for recording. Near the electrode placement areas, watches and jewelry were removed. Alcohol was used to clean the skin attachment sites of the electrodes. Subjects were seated upright and relaxed before recording. Typical cable configuration II was used to lay the cables. The negative electrode was placed on the palm side of the right forearm above the wrist, the positive electrode on the inner left leg just above the ankle, and the reference electrode on the inner right leg just below above the ankle Similar protocols were used to record the ECG data for all sessions. A total of 100 ECG signals with a duration of 1 min were collected from 50 participants (25 control and 25 experimental). The ECG signal acquisition procedure for the khat chewing portion of the study is shown in Figure 2.
Figure 2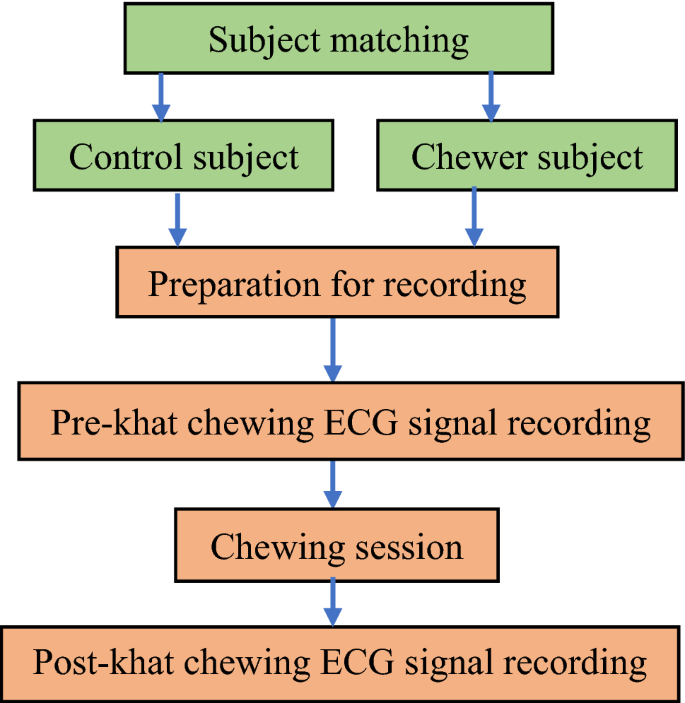
ECG data acquisition procedure to investigate the effect of khat chewing on cardiac activity.
For the khat addiction rehabilitation therapy portion of the study, data were obtained from khat addicts admitted to rehabilitation centers on the first day of admission and the eighth day of admission for each subject . Most of the subject addicted to khat recovers after a week stay in the rehabilitation program. At the rehabilitation center, participants used to take medications such as benzodiazepines, antidepressants or clonidine and therapies such as watching television, playing darts, playing table tennis, lifting weights, jumping rope and other sports activities recommended by the doctor. A case study approach was used for this part of the study. The sample size was limited to 5 because most subjects with other coaddictions, including alcohol, cigarettes, marijuana, opium, or a combination of one or more of these, were excluded from the study 10 ECG signals were recorded from these 5 subjects (1 female and 4 males), 5 before rehabilitation therapy and the remaining 5 after rehabilitation therapy.
The study was approved by the Institutional Review Board of the Jimma Institute of Health, University of Jimma, under permit number JHRPGN/75/21, and the Institutional Review Board of the Faculty of Medicine of the mil ·leni of the hospital of Saint Paul, with the approval number PM23/385. In addition, written informed consent was obtained from all study participants prior to data collection. All methods were conducted in accordance with the ethical standards set forth in the 1964 Declaration of Helsinki and its subsequent amendments or comparable ethical standards.
For the effect of khat on cardiac activity part of the study, data collection for control subjects and healthy chewers was conducted at Jimma University Medical Center according to their intuitive protocol. For the effect of khat addiction rehabilitation therapy on cardiac activity part of the study, data were collected at the psychiatric department of Saint Paul’s Millennium Medical College Hospital and rehabilitation center Addis Hiwot according to their respective protocols.
After signal imputation, all recorded ECG signals were annotated and denoised. Recorded signals were given a unique name to identify subject category, recording session, and count number. Low-frequency noises caused by respiratory muscle movement, temperature change, and electrode movement artifact were removed. The Savitzky Golay filter was used to smooth the signal and remove low-frequency disturbances20.
ECG signals are susceptible to disturbances such as power line interference, EMG noise, and electromagnetic interference, in addition to baseline abnormalities. As a result, unwanted noises must be removed before extracting the relevant features. For our purpose, a discrete wavelet transform that provides high performance to remove these noises from ECG signals21,22,23 was used for signal removal. Since the sampling frequency of the signals was 1000 Hz, the wavelet decomposition had frequency range patterns of 250–500 Hz, 125–251 Hz, 62.4–125 Hz, 31.2–62.6 Hz , 15.6–31.3 Hz, 7.79–7, . Hz, 1.95–3.92 Hz, 0.975–1.96 Hz, 0.487–0.979 Hz, 0.244–0.489 Hz, 0.0–0.243 Hz for detailed coefficients (D) D1, D2, D3, D4, D9 , D8, D6, D4 D10, D11 and approximate coefficient (A), respectively. Decomposition level 9 was used to remove frequency bands below 0.979 Hz assumed to be baseline stray noise. The wavelet noise-free signal was decomposed into wavelet coefficients, and the energy of each coefficient was calculated using a multi-resolution wavelet analysis (MRA) technique to remove residual noise. Low-frequency coefficients with a frequency range of less than 1 Hz that is outside the range of the ECG signal were excluded during wavelet reconstruction. Similarly, frequency coefficients in the ECG range with negligible energy contribution during reconstruction were excluded. As a result, the contribution coefficients from level 5 to level 9 were selected to reconstruct the noise signal.
Temporal peak detection and interval calculation techniques were used to calculate time domain ECG features, following the QRS detection approach of Pan Tompkins24. The Pan Tompkins algorithm is a time-domain QRS detection algorithm consisting of a series of low-pass filter, high-pass filter, derivative filter, square, threshold, and windowing procedures. Heart rate is calculated from the detected R peaks of the QRS complex. Figure 3 shows the feature extraction model employed in this study.
Figure 3
Feature extraction model.
The MATLAB peak detector functions “max” and “min” were used to detect the location and amplitude of the maximum and minimum peaks with the calculated moving time windows. The maximum and minimum amplitude points of each moving window were detected as R peaks and S peaks respectively. For the Q wave, the time window was between the left margin of the moving window and the location of the R peak, for the P wave between the left margin of the moving window and the location of the Q peak, and for the T wave between the location of the S peak and the right margin of the moving window. Intervals and segments were calculated from the start and offset points of each wave. The VFC was calculated using the root mean square of successive differences (RMSSD) between each peak R. Finally, all important calculated functions were exported to an excel format from the MATLAB workspace for further analysis .
The extracted features were averaged for better data manipulation. Changes between the mean before and after the chewing session were determined for both chewers and controls. Similarly, changes between mean values before and after rehabilitation therapy were determined and percentiles were calculated from these values. In addition, the results were statistically analyzed using a paired t test to show statistical differences between different groups (pre-chewing vs post-chewing of the experimental group, pre- vs post for the control group, pre-chewing of the experimental group ). vs the control and post-chewing session of the experimental group vs the control group).
A written informed consent form was obtained from all study participants.
[ad_2]Methadone Clinic Near Me – Methadone Clinic New York – Methadone Clinics USA














